Immunodeficiencies
Immunodeficiencies are disorders of the immune system that are characterized by a reduced or lack of ability to defend against microorganisms, i.e. bacteria, viruses and parasites. Immunodeficiencies are divided into primary (congenital and rare) and secondary (acquired and common).
Primary Immunodeficiencies
They constitute only approximately 5% of all immunodeficiencies. The more severe the immunodeficiencies, the earlier they appear, and the more severe their nature. Primary immunodeficiencies (PID) are a group of over 250 diseases whose essence is the improper functioning of some elements of the immune system. As a result, patients with primary immunodeficiency are much more likely to suffer from serious infections and suffer from many chronic diseases, mainly respiratory diseases. The biggest problem in Poland is still low awareness of the existence of PID and, consequently, a large number of undiagnosed patients. Untreated immune deficiencies can lead to serious chronic complications and even death of the patient.
Preprevalence of Primary Immunodeficiency (PID)
 Worldwide, approximately 1 in 10,000 people are affected by PIDs (2–5), a number which is likely underestimated due to “missed” diagnoses. The prevalence of the diseases varies greatly from country to country and is higher than this average in several countries.
Worldwide, approximately 1 in 10,000 people are affected by PIDs (2–5), a number which is likely underestimated due to “missed” diagnoses. The prevalence of the diseases varies greatly from country to country and is higher than this average in several countries.
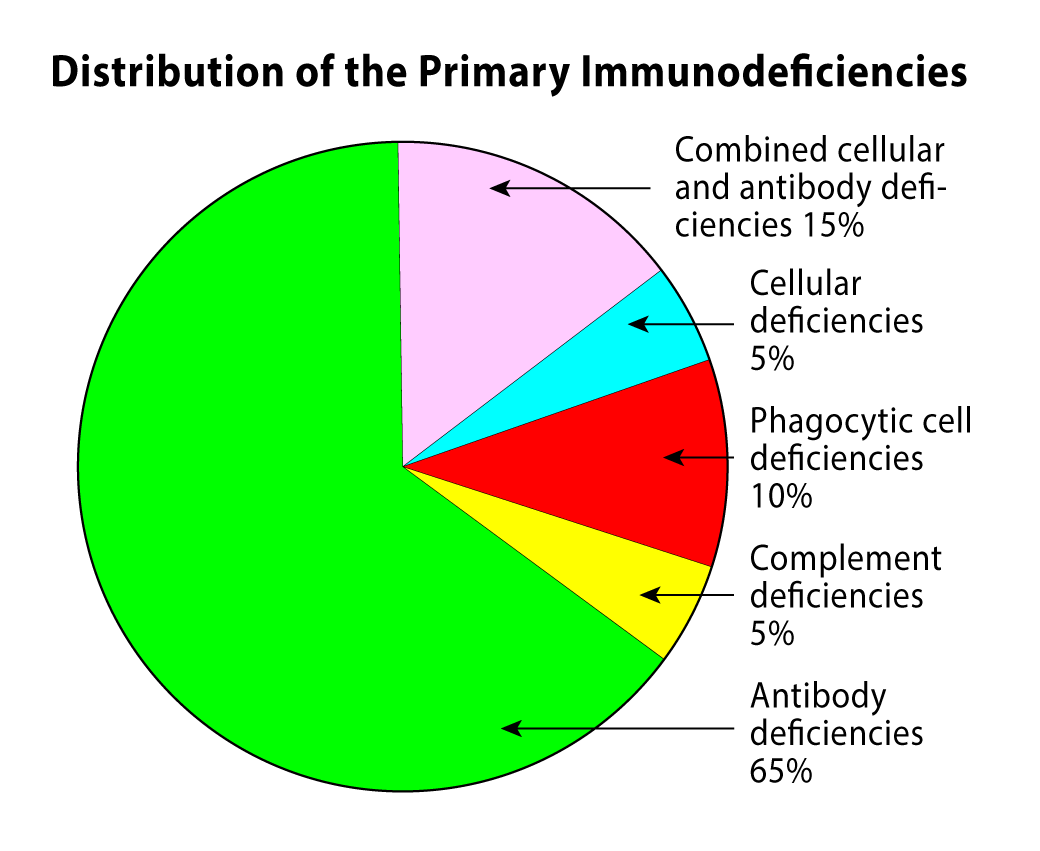
So far, almost 300 types of PIDs have been discovered, of which 55-65% of all types of primary immunodeficiencies are antibody deficiencies.
It is estimated that approximately 6 million people in the world probably suffer from Primary Immune Deficiencies.
57 % of Primary Immune Deficiencies are diagnosed among boys/men, and approximately 43 % among girls/women.
Minimum PID prevalence in the United Kingdom is currently 5,90/100 000 and an average incidence of PID between 1980 and 2000 of 7,6 cases per 100 000 UK live births.
Source: The United Kingdom Primary Immune Deficiency (UKPID) registry 2012 to 2017
Primary Immunodeficiency – Causes
Genetic mutations (changes) cause primary immunodeficiency. They are usually inherited, or passed down, within families, but can sometimes pop up sporadically. Providers treat primary immunodeficiency by preventing and managing infections and replacing missing or defective immune system components.
Primary Immunodeficiency – Symptoms
The most common symptoms of PID among children are chronic, recurrent infections and increased susceptibility to infections (especially of the respiratory tract). Skin infections, abscess formation and impaired wound healing are also common. Primary Immune Deficiencies may also be accompanied by autoimmune diseases, which are disturbances in the regulation of the human immune system (destruction of own cells and tissues). Such diseases include, for example: sarcoidosis, lupus erythematosus, psoriasis, rheumatoid arthritis or juvenile idiopathic arthritis, most often occurring in children with PID.
Some severe forms of primary immunodeficiencies produce symptoms that become apparent soon after birth. An example of such a condition is Di George syndrome, which causes facial deformities, heart disease and problems with the nervous system, which are observed at birth. Primary immunodeficiencies may also manifest themselves in autoimmune diseases, in which the body is attacked by its own immune system. This is manifested, for example, by a decrease in the number of platelets, arthritis or vitiligo. Most often, the first suspicions about the occurrence of PID arise from serious infections. These are usually severe, recurrent infections that are difficult to treat despite the use of antibiotics. If we suffer from inflammation of the ears, sinuses, bronchi or lungs once again during the year, we should not underestimate it, because it may be a signal that our immune system is not functioning properly.
Primary Immunodeficiency – Diagnosis
When PID is suspected, more detailed tests of the immune system are performed. – They are usually performed gradually to exclude the most severe forms of PID, such as severe combined immunodeficiency (SCID), at the very beginning. First, a blood count with a smear is performed, and then - if necessary - immunoglobulin levels are determined and a number of other specialist tests are performed. A complete blood count is the main indicator of abnormalities related to the immune system, but it is not sufficient to properly diagnose primary immunodeficiency. Blood count results are rather an indication for more accurate tests for specific cell types. Such tests are usually performed by immunologists.
If the patient is diagnosed with an immune deficiency, appropriate treatment may be initiated. Although PID cannot be completely cured, effective therapies improve the health of sick people, significantly reduce the number of infections and allow them to lead an active life, develop a professional career and have a family. The most common method of treatment is immunoglobulin replacement therapy, i.e. subcutaneous or intravenous administration of human immunoglobulin preparations, in most patients throughout their lives.
The list of 10 warning symptoms suggestive of the disease among children, developed by experts from the European Immunodeficiency Society and the Jeffrey Modell Foundation, is helpful in diagnosing Primary Immunodeficiencies. The occurrence of 2 of the 10 symptoms described above should be a disturbing indication that the doctor may suspect that the patient has one of the Primary Immunodeficiencies.
Warning symptoms that may suggest primary immunodeficiencies in children
- Four or more ear infections (inflamations) within a year
- Two or more sinus infections in a year
- Antibiotic therapy for 2 months or longer with little improvement
- Two or more pneumonias in a year
- No weight gain, stunted growth
- Recurrent deep skin or organ abscesses
- Chronic oral or skin mycosis in children after 1 year of age
- The need for long-term treatment of the infection with intravenous antibiotics
- Two or more serious infections such as sepsis, inflammation of the brain, bones, skin
- Family history indicating the occurrence of PID
Primary Immunodeficiency – Therapy
Treatment must go in two directions (1) be directed at treating the deficiencies as far as possible and (2) combating infections and other diseases resulting from immune deficiencies.
Managing infections
• Treating infections. Infections require rapid and aggressive treatment with antibiotics. Treatment might require a longer course of antibiotics than is usually prescribed. Infections that don't respond may require hospitalization and intravenous (IV) antibiotics.
• Preventing infections. Some people need long-term antibiotics to prevent respiratory infections and permanent damage to the lungs and ears. Children with primary immunodeficiency might not be able to have vaccines containing live viruses, such as oral polio and measles-mumps-rubella.
• Immunoglobulin therapy. Immunoglobulin consists of antibody proteins needed for the immune system to fight infections. It can either be injected into a vein through an intravenous (IV) line or inserted underneath the skin (subcutaneous infusion). treatment is needed every few weeks, and subcutaneous infusion is needed once or twice a week.
Treatment to reinstitute the immune system
• Stem cell transplantation. Stem cell transplantation offers a permanent cure for several forms of life-threatening immunodeficiency. Normal stem cells are transferred to the person with immunodeficiency, which results in a typically functioning immune system. Stem cells can be harvested through bone marrow, or they can be obtained from a placenta at birth (cord blood banking). The stem cell donor — usually a parent or other close relative — must have body tissues that are a close biological match to those of the person with primary immunodeficiency. Even with a good match, however, stem cell transplants don't always work. The treatment often requires that functioning immune cells be destroyed using chemotherapy or radiation before the transplants, leaving the transplant recipient temporarily even more vulnerable to infection.
In the case of the most severe immune deficiencies, such as SCID (severe combined immunodificiency), bone marrow transplantation is used.
• Gene therapy. This type of treatment involves taking stem cells from the person with primary immunodeficiency, correcting the gene in the cells and then returning the corrected stem cells back to the person via an intravenous infusion. With gene therapy, there is no need to find a suitable donor, as the person's own cells are used. Currently, this treatment is used to treat only a few primary immunodeficiencies, but clinical trials are underway for many other types.
Typically, patients with primary immunodeficiencies must take medications for the rest of their lives, but this does not prevent them from functioning normally. A person with PID can and should lead a normal life. There are no contraindications for her to go to school, study or work. Of course, you need to remember to take certain precautions to minimize the risk of infection, but that's basically it.
It should be noted that in the case of primary immunodeficiencies, the diagnosis of the disease and the directions of treatment should be determined by an immunologist, and the therapy is carried out on a daily basis by a family doctor.